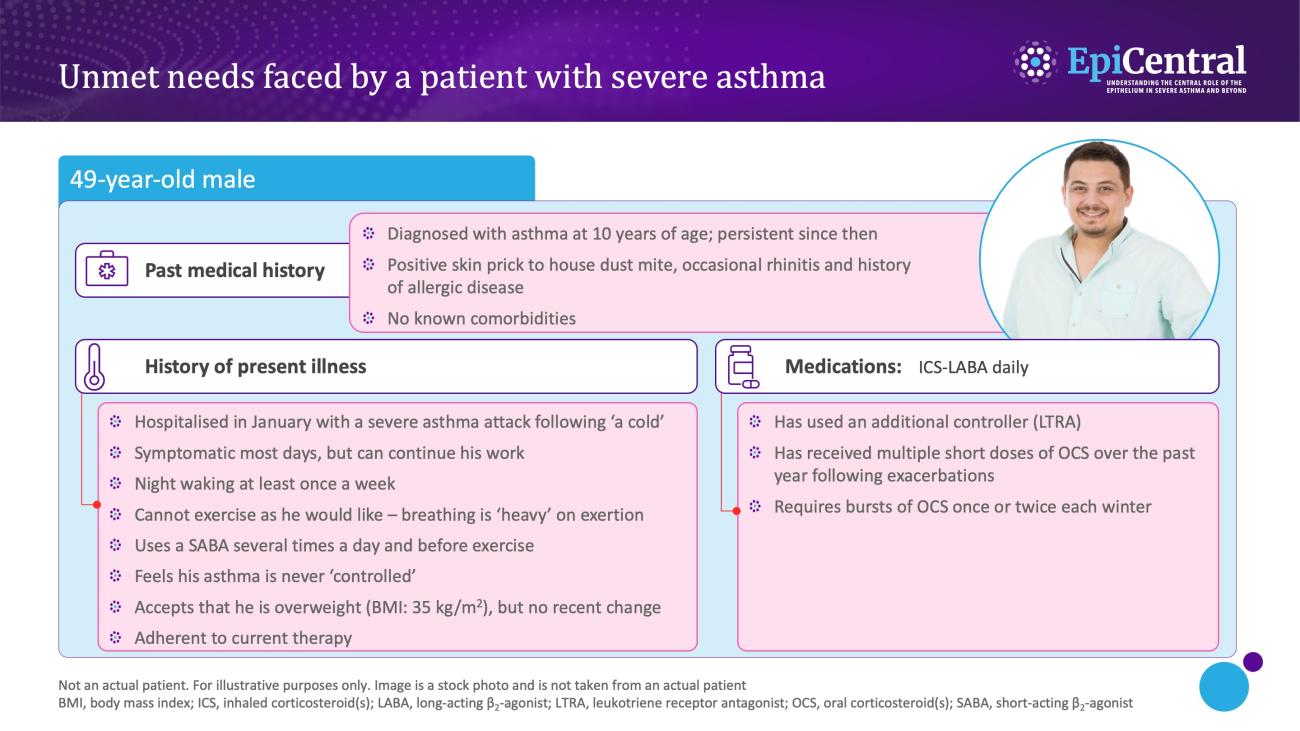
The long-term goals of severe asthma management include achieving good symptom control and minimising the future risk of exacerbations and disease progression (eg, decline of lung function and persistent airflow limitation).2 In many cases where patients have poor symptom control and/or exacerbations despite medium- or high-dose ICS and LABA therapy, their asthma may appear difficult to treat because of contributory factors, such as incorrect inhaler technique, poor adherence, smoking or comorbidities, or because of incorrect diagnosis.2 For these patients, GINA recommends assessment of these contributory factors and consideration of an add-on therapy, eg, a long-acting muscarinic antagonist (LAMA).2 If problems persist, referral to a specialist centre for phenotypic assessment and consideration for add-on biologic targeted treatments are recommended.2
Confirming the diagnosis of asthma, assessing contributory factors and optimising treatment strategy are the key steps for consideration in the diagnosis and management of severe asthma.2
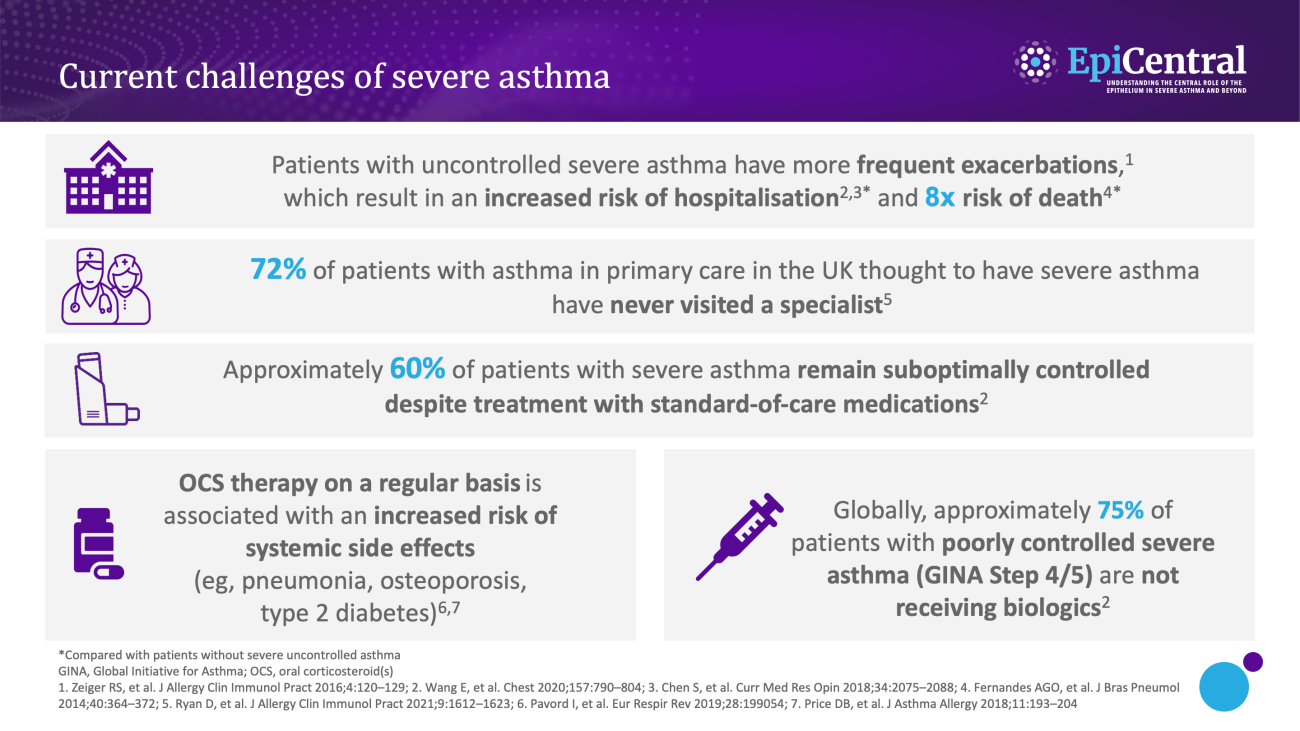
To date, there has been great progress in the diagnosis and management of severe asthma,5,6 with biologics representing a major advancement in the treatment landscape.7 However, many patients with severe asthma are poorly controlled.
A recent study found that approximately 60% of patients with severe asthma remained suboptimally controlled despite treatment with standard-of-care medications.8 This significant finding was described following a retrospective and prospective analysis of the International Severe Asthma Registry – a data set of 4990 patients receiving GINA Step 5 treatment or with severe asthma remaining uncontrolled at GINA Step 4 (December 2014 to December 2017). Poorly controlled asthma was defined in this study according to Asthma Control Test (score 5–15; ‘very poorly controlled’) or Asthma Control Questionnaire (score >1.5; ‘poorly controlled’) categorisations.8